
Publications
2026
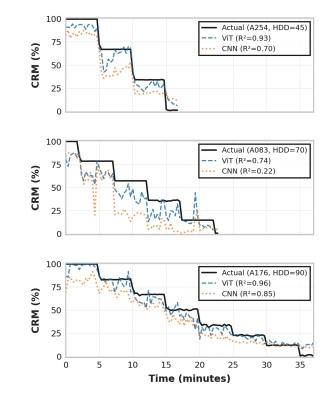
Tibbs, M. L., McCloskey, B., Snider, E. J., Convertino, V. A., & Petersen, L. G. (2026). Breaking the Black Box: Interpretable AI Achieves Superior Hemorrhage Detection with the Compensatory Reserve Measurement. IEEE Journal of Biomedical and Health Informatics, 1–14. https://doi.org/10.1109/JBHI.2026.3690009
ABSTRACT: Hemorrhage remains the leading cause of preventable trauma death, with traditional vital signs failing to detect blood loss until 25-30% volume depletion occurs. Compensatory Reserve Measurement (CRM) enables earlier hemorrhage detection but current estimation methods force a tradeoff between performance and interpretability. We present the first Vision Transformer (ViT) for CRM estimation that achieves both superior accuracy compared to previous models and mechanistic explainability from arterial blood pressure (ABP) waveforms. Using data from 208 human subjects who underwent progressive lower body negative pressure, we developed a single-layer ViT that processes 20-second waveform segments as token sequences. Rigorous 10-fold cross-validation compared the ViT against state of-the-art Convolutional Neural Network (CNN) and manual feature-based models using identical train-validation-test splits. With all models undergoing equivalent Optuna hyperparameter optimization, the ViT achieved higher R2 (0.80 vs 0.77) with fold-level paired t-test p = 0.052 (N = 10) and subject-level p = 0.008 (N = 208). The ViT also demonstrated superior robustness to signal corruption, with the CNN’s performance degrading progressively faster under increasing noise and sample dropout. Attention analysis revealed learned patterns converging with established physiological knowledge, prioritizing half-decay and dicrotic notch regions identified as critical by manual feature extraction from the ABP. The model shifted from focused attention at high CRM to distributed monitoring at low CRM, matching known hemodynamics near decompensation. Ablation experiments confirmed half-decay regions as functionally critical. This work bridges the performance-interpretability tradeoff, providing the first interpretable deep learning approach for hemorrhage monitoring and CRM estimation.
Tibbs, M. L., Lee, C., Morse, B. G., Romero, E., & Petersen, L. G. (2026). In-Flight Assessment of Simulated Hemorrhage During Aerial Patient Evacuation. Aerospace Medicine and Human Performance, 97(2), 123–130. https://doi.org/10.3357/AMHP.6768.2026
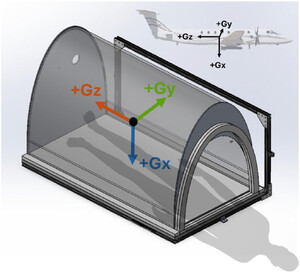
INTRODUCTION: Understanding how flight trajectories impact hemodynamically unstable patients is critical for maintaining high survival rates during aerial evacuation. We integrated an experimental model of hemorrhage in an aircraft during evasive maneuvers to capture the physiological response in healthy humans vs. simulated hemorrhage.
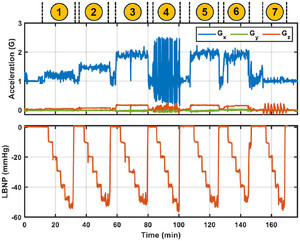
METHODS: Lower body negative pressure (LBNP), a validated method to simulate hemorrhage, and continuous physiological monitoring were integrated into a C-12J aircraft. Nine volunteers underwent incremental LBNP during wind-up turns, roller coasters, and level acceleration/deceleration trajectories at cabin pressure altitudes of 5500–9500 ft (1670–2890 m). Environmental sensors recorded acceleration, vibration, temperature, and pressure.
RESULTS: Nine sorties totaling 27.5 flight test hours were completed. Wind-up turns produced Gx accelerations of 1.21 ± 0.09 G (mean ± SD), 1.47 ± 0.06 G, and 1.93 ± 0.10 G, with additional Gz (0.05–0.18 G). Roller coasters produced rapid Gx transitions between 0.4–2.8 G. Level acceleration/decelerations generated −0.1–0.3 Gz. Incremental LBNP was applied from 0–60 mmHg, simulating mild, moderate, and severe hemorrhage. Gx was driven by low-frequency aerodynamics; lateral by high-frequency mechanical inputs.
DISCUSSION: We have, for the first time, established a real-world in-flight experimental set-up to conduct direct crossover trials and capture the reductions in Gx-tolerance and vibration between healthy and hemodynamically unstable patients. Our method allows us to titrate LBNP level (degree of hemorrhage) and G-forces independently, thus providing a tool to understand both isolated and synergistic impact of acceleration and blood-loss to establish dose-response relationships. Our method provides important human data to directly quantify the delta between healthy human and simulated trauma (hemorrhage) to better understand the underlying mechanisms of cardiovascular decompensation in casualty evacuation.
2025
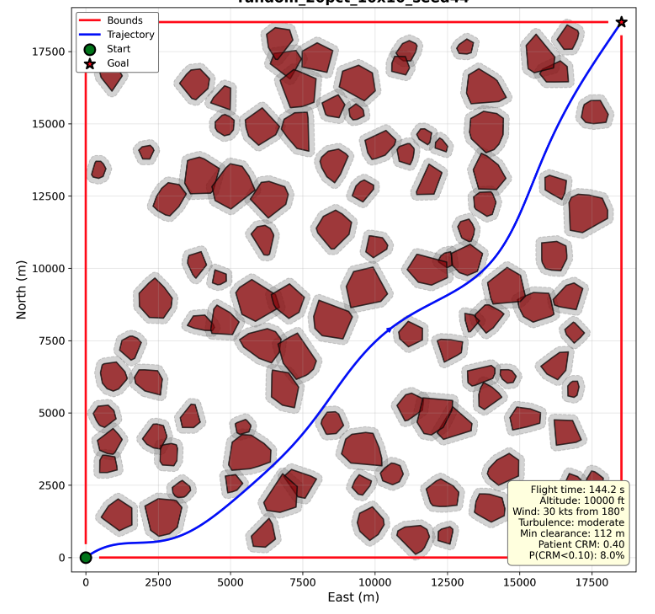
Tibbs, M., Balakrishnan, H., & Petersen, L. (2025). Physiologically-constrained trajectory optimization for autonomous medical air transport. 2025 AIAA DATC/IEEE 44th Digital Avionics Systems Conference (DASC). Presentation only.
Tibbs, M. L., Morse, B. M., Siu, H. C., & Petersen, L. G. (2025). Transformer vs. Manual Feature Engineering of Arterial Waveforms for Forecasting Hemodynamic Responses to Combined G-Force and Hemorrhage. Annual International Conference of the IEEE Engineering in Medicine and Biology Society. IEEE Engineering in Medicine and Biology Society. Annual International Conference, 2025, 1–7. https://doi.org/10.1109/EMBC58623.2025.11254404
ABSTRACT: In the face of increased and more severe natural disasters around the world, future civilian and military medical evacuation (MEDEVAC) operations may require aggressive flight maneuvers, subjecting hemodynamically unstable casualties to potentially dangerous G-forces. Moreover, there are limited data and no known prediction models available to understand the physiological effects. Therefore, this paper presents the first set of models and a comparative analysis of transformer-based and traditional feature engineering approaches for forecasting hemodynamic responses under concurrent hemorrhage and G-force exposure. We developed a cross-dataset transfer learning framework using a modified Vision Transformer pre-trained on MIMIC-IV arterial blood pressure (ABP) waveform data and fine-tuned on experimental data that combines lower body negative pressure to simulate hemorrhage with centrifuge-induced G-force. Comparing zero-shot and fine-tuned transformer features against manually engineered ABP features, we found that while manual features achieved marginally better performance for forecasting systolic blood pressure (MSE: 30.19 ± 16.31 mmHg2, R2: 0.84 ± 0.09), the fine-tuned transformer approach demonstrated comparable results (MSE: 32.43 ± 19.43 mmHg2, R2: 0.82 ± 0.11) with no statistically significant difference. Principal component analysis revealed that manually engineered features captured more variance in fewer dimensions, while learned features showed promise in distinguishing between physiological conditions. This work establishes benchmarks for physiological forecasting under combined stressors and provides a foundation for developing autonomous MEDEVAC systems for operations in hostile environments.Clinical Relevance— Predicting hemodynamic responses under concurrent hemorrhage and G-force exposure may support the development of autonomous patient monitoring systems that improve real-time decision-making and casualty outcomes for medical air transport.
Morse, B., Tibbs, M., Petersen, L., & Petersen, C. (2024). MODELING THE IMPACT OF FLIGHT CONDITIONS ON PULMONARY FUNCTION IN TRANSPORTED CASUALTIES TO FACILITATE FUTURE UNMANNED CASEVAC SAFETY. Aerospace Medicine & Human Performance, 95(8). https://search.ebscohost.com/login.aspx?direct=true&profile=ehost&scope=site&authtype=crawler&jrnl=23756314&AN=178876174&h=v3dHlfdngb%2FwRAX%2Bw16PXon6rmRz4LAamUMAyM3CCIqqZ2yAizEGmLhZ4sYFwwCaIbyWtJB%2BBUGk%2F9tEoXBo9g%3D%3D&crl=c
ABSTRACT: It is anticipated that commanders will want to reduce the risk to personnel in future military theaters by employing unpiloted aerial vehicles (UAV) in combat zones. Evasive maneuvering required for casualty evacuation in contested environments can expose patients to flight conditions and forces that It is anticipated that commanders will want to reduce the risk to personnel in future military theaters by employing unpiloted aerial vehicles (UAV) in combat zones. Evasive maneuvering required for casualty evacuation in contested environments can expose patients to flight conditions and forces that put their health at risk. Pulmonary function is highly susceptible to gravitational impact. Although it is known that hypergravity and hemorrhagic blood loss are factors that can independently lead to atelectasis, the combined and potentially synergistic impact of these two factors remains unknown. This study aimed to assess the feasibility of developing pulmonary models to identify threshold values for when hemorrhagic patients begin having difficulty tolerating gravitational G-force-related stress. METHODS: The study was approved by the AFRL IRB. Six healthy volunteers (two female, age 33±10 years) were placed supine inside the centrifuge. Moderate hemorrhage was simulated by -20 mmHg LBNP. Evasive maneuvers were simulated by 15-sec 4Gx acceleration in isolation and in combination with LBNP. Electrical impedance tomography (EIT) (Enlight 2100, Timpel Medical, Brazil) was used to measure changes in ventilatory distribution at the 4th and 5th intercostal spaces. RESULTS: LBNP alone had limited impact on air distribution within the lungs, while the Gx-only condition contributed to a shift in ventilation towards the anterior portion of the lungs. However, the data indicate that the combination of Gx and hemorrhage further exaggerates the lung’s uneven posterior and anterior air distribution. DISCUSSION: The data suggests that supine exposure to Gx elicits a disturbance in the lung’s ventilation-perfusion relationship. The apparent further exacerbation of this mismatch in simulated hemorrhage conditions should be considered in future models used to create safe and robust autonomous flight-restraint systems for UAV-CASEVAC. Learning Objectives 1. Evasive flight maneuvers (steep bank) can lead to uneven air distribution in the lungs, increasing the risk of atelectasis for patients with mild/moderate blood volume loss. 2. To aid in the initial investigation of mapping physiological data to suitable flight envelopes and trajectories. put their health at risk. Pulmonary function is highly susceptible to gravitational impact. Although it is known that hypergravity and hemorrhagic blood loss are factors that can independently lead to atelectasis, the combined and potentially synergistic impact of these two factors remains unknown. This study aimed to assess the feasibility of developing pulmonary models to identify threshold values for when hemorrhagic patients begin having difficulty tolerating gravitational G-force-related stress. METHODS: The study was approved by the AFRL IRB. Six healthy volunteers (two female, age 33±10 years) were placed supine inside the centrifuge. Moderate hemorrhage was simulated by -20 mmHg LBNP. Evasive maneuvers were simulated by 15-sec 4Gx acceleration in isolation and in combination with LBNP. Electrical impedance tomography (EIT) (Enlight 2100, Timpel Medical, Brazil) was used to measure changes in ventilatory distribution at the 4th and 5th intercostal spaces. RESULTS: LBNP alone had limited impact on air distribution within the lungs, while the Gx-only condition contributed to a shift in ventilation towards the anterior portion of the lungs. However, the data indicate that the combination of Gx and hemorrhage further exaggerates the lung’s uneven posterior and anterior air distribution. DISCUSSION: The data suggests that supine exposure to Gx elicits a disturbance in the lung’s ventilation-perfusion relationship. The apparent further exacerbation of this mismatch in simulated hemorrhage conditions should be considered in future models used to create safe and robust autonomous flight-restraint systems for UAV-CASEVAC. Learning Objectives 1. Evasive flight maneuvers (steep bank) can lead to uneven air distribution in the lungs, increasing the risk of atelectasis for patients with mild/moderate blood volume loss. 2. To aid in the initial investigation of mapping physiological data to suitable flight envelopes and trajectories.
Petersen, L., Morse, B., Tibbs, M., & Petersen, C. (2024). UAV FOR CASUALTY TRANSPORT: QUANTIFYING REDUCTION IN G-TOLERANCE IN HEMORRHAGIC PATIENTS. Aerospace Medicine & Human Performance, 95(8), 464.
ABSTRACT: Future CASEVAC will likely include Unpiloted Aerial Vehicles (UAV) for casualty-transport (drone-ambulances) from combat-zones. Elimination of human-in-the-loop with regards to pilot and medical personnel to monitor flight-impact on patients increases the risk of inadvertent unsafe flight maneuvers. It is presumed that G-tolerance is reduced in casualty, particularly relative to blood-loss, however, we have no physiological data to quantify this reduction. We used long-arm human centrifuge to simulate evasive flight maneuvers ( Gx) and a custom-built lower body negative pressure (LBNP) device to simulate hemorrhage in a controlled and reversible way. METHODS: The study was approved by the AFRL IRB. Six healthy volunteers (two female, age 33±10 years) were placed supine inside the centrifuge. Moderate hemorrhage was simulated by -20 mmHg LBNP. Evasive maneuvers were simulated by 15-sec 4Gx acceleration in isolation and in combination with LBNP. Mean arterial pressure (MAP) and stroke volume (SV) were collected using Nexfin (BMEye). Delta values were analyzed using RM-ANOVA and Šídák’s multiple comparisons test. RESULTS: Blood pressure was not reduced by LBNP alone (DMAP= -3.4±7.4 mmHg; P=0.8). Gx alone significantly reduced MAP (DMAP= -19.4±11.4 mmHg; P0.05), however, combined effect of LBNP Gx significantly reduced SV (DSV= -24.2±13.0 mL; P=0.0019). Synergistic effect of hemorrhage and G-load reduced SV to an absolute value of 78.0±19.4 mL. DISCUSSION: These data indicate a synergistic effect between Gx maneuvers and simulated hemorrhage which was significantly more pronounced than either intervention in isolation. Understanding and quantifying G-tolerance of casualties is critical to create safe autonomous flightrestraint systems for UAV-CASEVAC. Learning Objectives 1. Evasive flight maneuvers (steep bank) simulated by short periods of 4Gx can lead to severe reduction in MAP in patients with mild/moderate blood volume loss. 2. Qualitative and quantitative mapping of physiology is critical to develop suitable flight envelopes and trajectories.